







Quick Links
- Why does keratoconus occur?
- Symptoms of Keratoconus
- What Causes Keratoconus?
- How Keratoconus Is Diagnosed
- Keratoconus Treatment Options
- Why Early Keratoconus Treatment Matters
- Can Keratoconus Cause Blindness?
- Who Is at Higher Risk?
- Personalized Keratoconus Treatment Approach
- What to Expect During Treatment
- Great External Resources
- Frequently Asked Questions (FAQs)
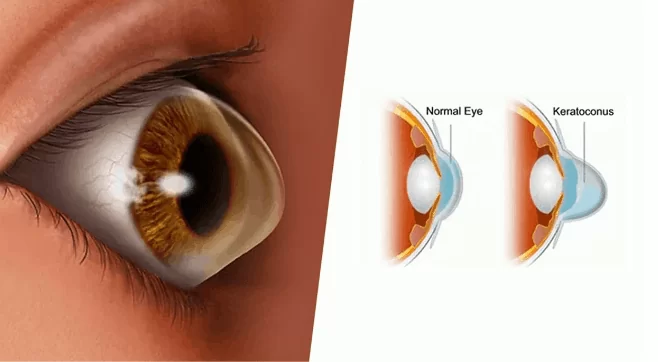
What Is Keratoconus?
Keratoconus is a progressive eye condition that affects the cornea — the clear, dome-shaped front surface of the eye responsible for focusing light. In healthy eyes, the cornea maintains a smooth, round curvature. In keratoconus, the corneal structure weakens and gradually thins, causing it to bulge outward into a cone-like shape.
As the cornea becomes irregular, light entering the eye is distorted. This leads to blurred vision, glare, halos around lights, increasing nearsightedness, and irregular astigmatism that cannot be fully corrected with glasses alone.
Keratoconus typically begins in the teenage years or early twenties and may progress over 10–20 years. Early detection and timely keratoconus treatment are critical to preserving vision and preventing long-term complications.

Symptoms of Keratoconus
Keratoconus often develops gradually. In its early stages, symptoms may be subtle and easily mistaken for simple vision changes.
Common signs include:
Blurred or distorted vision
Frequent changes in glasses prescription
Increased sensitivity to light
Glare and halos around lights, especially at night
Double vision in one eye
Difficulty driving at night
Progressive worsening of astigmatism
As the condition advances, vision may become significantly distorted, and glasses may no longer provide adequate correction.

What Causes Keratoconus?
The exact cause of keratoconus is not fully understood, but research suggests a combination of genetic, environmental, and biochemical factors.
Risk factors may include:
Family history of keratoconus
Chronic eye rubbing
Allergies, asthma, or eczema (atopic conditions)
Connective tissue disorders
Hormonal influences (including pregnancy-related progression)
Eye rubbing is considered a major contributing factor, as it may accelerate corneal weakening.
How Keratoconus Is Diagnosed
Early diagnosis plays a vital role in successful keratoconus treatment. Advanced diagnostic technology allows detection even before symptoms become severe.
1. Refraction Test
Measures visual clarity and determines prescription strength.
2. Slit-Lamp Examination
Allows detailed evaluation of the cornea using magnified light.
3. Keratometry
Measures the curvature of the cornea.
4. Corneal Topography and Tomography
Creates a detailed color-coded map of the corneal surface. These scans can detect early changes long before they are visible through routine examination.
Corneal thickness measurement (pachymetry) is also essential, as thinning is a hallmark of keratoconus.
Keratoconus Treatment Options
Keratoconus treatment depends on:
Severity of the condition
Rate of progression
Corneal thickness
Visual needs of the patient
Treatment generally focuses on two goals:
Stopping progression
Improving vision
Below are the most effective modern keratoconus treatment options available today.
1. Glasses and Soft Contact Lenses (Early Stage)
In the earliest stages, glasses or soft contact lenses can effectively correct mild nearsightedness and astigmatism.
However, as keratoconus progresses and irregular astigmatism increases, glasses may no longer provide clear vision.
2. Rigid Gas Permeable (RGP) Contact Lenses
When irregularity increases, rigid contact lenses become the next step.
These lenses:
Provide a smooth refractive surface
Mask corneal irregularity
Significantly improve visual clarity
Although they may require an adaptation period, many patients achieve excellent vision with properly fitted rigid lenses.
Other specialized lens options include:
Hybrid lenses (rigid center, soft outer ring)
Piggyback lenses (rigid lens over soft lens)
Scleral lenses (vault over the cornea and rest on the sclera)
Scleral lenses are particularly effective in advanced keratoconus because they do not touch the cornea directly.
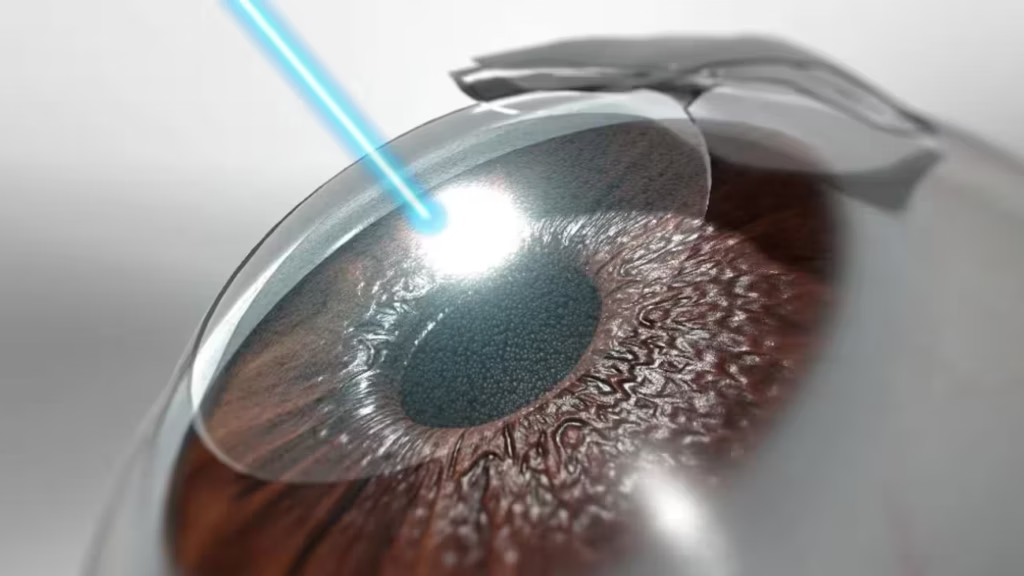
3. Corneal Collagen Cross-Linking (CXL)
Corneal cross-linking is one of the most important advancements in keratoconus treatment.
What Is Cross-Linking?
This minimally invasive procedure strengthens the cornea by increasing collagen bonds within the corneal tissue.
How It Works:
- Riboflavin (Vitamin B2) eye drops are applied to the cornea
- The eye is exposed to controlled ultraviolet-A (UVA) light
- The interaction strengthens the collagen fibers
Benefits:
- Slows or stops disease progression
- Reduces risk of corneal transplant
- Stabilizes vision
- May slightly improve corneal shape
Cross-linking is most effective when performed early, before severe thinning occurs.
4. Intracorneal Ring Segments (ICRS)
Intracorneal ring segments are small, arc-shaped implants inserted into the cornea to improve its shape.
Purpose:
Flatten the steep corneal cone
Reduce irregular astigmatism
Improve contact lens tolerance
Enhance visual quality
These rings:
Are removable
Do not replace corneal tissue
Can delay or prevent the need for transplant
Modern techniques use femtosecond laser technology to create precise channels, increasing safety and accuracy.
5. Topography-Guided PRK (Selective Cases)
In selected patients, topography-guided surface laser treatment may be used to smooth corneal irregularity.
Important considerations:
Only minimal tissue is removed
Usually combined with corneal cross-linking
Not designed to eliminate glasses entirely
Suitable only when corneal thickness allows
This approach aims to improve quality of vision rather than provide full refractive correction.
6. Implantable Collamer Lens (ICL)
For patients with very high myopia or astigmatism who achieve reasonable clarity with glasses but have extreme prescriptions, implantable lenses inside the eye may be considered.
These lenses:
Correct high refractive errors
Are placed behind the iris
Do not treat the corneal shape directly
They are suitable only in carefully selected cases.
7. Corneal Transplant (Advanced Cases)
In severe keratoconus with:
Significant scarring
Extreme thinning
Poor vision despite lenses
Inability to tolerate contact lenses
A corneal transplant may be recommended.
1. Partial Thickness (DALK)
Replaces only the front layers of the cornea while preserving healthy inner layers.
2. Full Thickness (Penetrating Keratoplasty)
Replaces the entire cornea with donor tissue.
Modern techniques improve precision and reduce rejection risks. Corneal transplantation is among the most successful transplant procedures worldwide.
Why Early Keratoconus Treatment Matters
Delaying treatment can lead to:
Permanent corneal scarring
Severe thinning
Increased risk of transplant
Irreversible vision loss
Early intervention, particularly with corneal cross-linking, can stabilize the disease and protect long-term vision.
Can Keratoconus Cause Blindness?
While keratoconus rarely causes complete blindness, untreated progression can result in severe vision impairment. Fortunately, with modern keratoconus treatment options, most patients maintain functional vision throughout their lives.
Who Is at Higher Risk?
You may be at increased risk if you:
Have a family history of keratoconus
Frequently rub your eyes
Have chronic allergies
Have asthma or eczema
Are between ages 10–30
Routine eye examinations are especially important for high-risk individuals.
Personalized Keratoconus Treatment Approach
No two corneas are the same. Effective keratoconus treatment requires:
Advanced diagnostic imaging
Careful assessment of corneal thickness
Evaluation of progression rate
Customized treatment planning
A personalized approach ensures the safest and most effective outcome.
What to Expect During Treatment
Most procedures are:
Outpatient
Performed under local anesthesia
Minimally invasive
Associated with short recovery times
Follow-up visits are essential to monitor healing and stability.
Great External Resources
Frequently Asked Questions (FAQs)
Why does keratoconus occur?
It occurs when the cornea — the clear front surface of the eye — becomes progressively thinner and weaker. This structural weakness causes the cornea to bulge outward into a cone-like shape. The exact cause is not fully understood, but research suggests a combination of genetic, environmental, and biochemical factors. It often runs in families, indicating a hereditary link. Chronic eye rubbing is strongly associated with progression, as it may damage collagen fibers within the cornea. Allergies, asthma, eczema, and certain connective tissue conditions are also linked. Hormonal influences, including pregnancy, may contribute to progression in some individuals.
Why is keratoconus bad?
It is concerning because it causes progressive distortion of vision. As the cornea becomes irregular, light entering the eye cannot focus properly on the retina, leading to blurred and distorted vision. Glasses may no longer correct vision effectively due to irregular astigmatism. Over time, untreated keratoconus can lead to severe thinning, corneal scarring, and significant visual impairment. In advanced stages, patients may struggle with daily activities such as driving or reading. While it rarely causes total blindness, it can substantially affect quality of life if not monitored and treated early with appropriate keratoconus treatment options.
Why does keratoconus cause headaches?
It can cause headaches because the eyes must constantly strain to focus through an irregularly shaped cornea. The distorted corneal surface leads to blurred or fluctuating vision, forcing the visual system to work harder to achieve clarity. This prolonged eye strain may result in tension headaches, especially after reading, screen use, or driving. Additionally, increased light sensitivity and glare can contribute to visual fatigue. Frequent prescription changes may also make it difficult for the brain to adapt to visual correction. Proper diagnosis and appropriate visual correction, such as specialty contact lenses, often reduce headache symptoms significantly.
Why does keratoconus cause myopia?
It causes myopia (nearsightedness) because the cornea becomes steeper as it bulges into a cone shape. A steeper cornea bends light more strongly than normal, causing light rays to focus in front of the retina instead of directly on it. This results in blurry distance vision while near objects remain clearer. As the condition progresses and the corneal curvature increases further, myopia may worsen rapidly. This is why individuals with keratoconus often require frequent prescription updates. In addition to myopia, irregular astigmatism develops, making standard glasses less effective over time.
Why is my keratoconus getting worse?
It typically progresses during the teenage years and young adulthood. Progression occurs because the corneal collagen fibers continue to weaken, allowing further thinning and bulging. Risk factors such as frequent eye rubbing, uncontrolled allergies, and hormonal changes may accelerate progression. In some individuals, the condition naturally advances for 10–20 years before stabilizing. If your vision is worsening, it may indicate ongoing corneal steepening. Early intervention with corneal collagen cross-linking can help halt progression and preserve vision. Regular corneal imaging is essential to detect subtle changes before significant visual loss occurs.
Why can't I wear glasses with keratoconus?
In early stages, glasses can correct vision effectively. However, as keratoconus progresses, the cornea becomes irregular rather than uniformly curved. Glasses correct regular refractive errors but cannot fully compensate for irregular astigmatism caused by corneal distortion. This leads to persistent blurriness, ghosting, or shadowing even with updated prescriptions. Specialty contact lenses — such as rigid gas permeable or scleral lenses — create a smooth optical surface over the cornea, significantly improving clarity. Therefore, difficulty with glasses usually indicates that the condition has advanced beyond mild stages.
Will keratoconus cause blindness?
It rarely causes complete blindness. However, if left untreated and allowed to progress significantly, it can result in severe visual impairment. Advanced thinning, scarring, or corneal rupture (a rare complication called acute hydrops) may substantially reduce vision. Fortunately, modern keratoconus treatment options — especially corneal cross-linking — can halt progression in most patients when performed early. Even in advanced cases, specialty contact lenses or corneal transplantation can restore functional vision. With proper monitoring and timely treatment, most individuals maintain useful vision throughout their lives.
Will keratoconus get worse?
It is generally a progressive condition, particularly in younger individuals. It often worsens over 10 to 20 years before stabilizing naturally. The rate of progression varies widely; some people experience rapid changes, while others have slow or minimal progression. Factors such as age, genetics, and eye rubbing habits can influence how quickly it advances. Early diagnosis and treatment, particularly with corneal cross-linking, significantly reduce the risk of further deterioration. Regular follow-up examinations are essential to monitor changes in corneal shape and thickness.
Will keratoconus make me blind?
While it can cause serious vision problems, it is very unlikely to cause total blindness. Most patients retain functional vision with appropriate treatment and visual correction. In advanced stages, severe distortion or scarring may make daily activities difficult, but treatment options such as scleral lenses or corneal transplantation can often restore clarity. The key factor is early detection and proactive management. Modern advancements in keratoconus treatment have greatly reduced the risk of severe, irreversible vision loss.